Beyond Hospitals: Rethinking Where Emerging Infectious Disease Threats Begin.
The first case is almost never the first case.
By the time an emerging infectious disease produces a patient sick enough to reach a clinic, and unusual enough for someone to realise this is not the usual fever, the pathogen behind it has often been moving for weeks, months, sometimes years. It may have slipped from an animal into a person through zoonotic spillover, passed quietly between households, or crossed a border inside someone who never felt unwell. When the test result finally comes back, it does not mark the beginning of the outbreak. It marks the moment we noticed.
We have built a century of public health around that moment. Hospitals and laboratories are extraordinary at confirming, naming and treating disease once it arrives. What they cannot do is see it coming, and increasingly, seeing it coming is the part that matters most.
This is not a failure of medicine. It is a failure of where we have chosen to look. If the first place we search for tomorrow’s outbreak is the clinic, we will always be searching late. The more demanding question, and perhaps the more hopeful one, is whether we can learn to look upstream: in the forests, farms, wetlands and shifting landscapes where new diseases actually begin, and where, more often than we like to admit, we are the ones setting them in motion.
So: are we looking for the next outbreak in the right places?
What is zoonotic spillover?
Most “new” human diseases are not new at all. They are old animal infections that have found a fresh host: us. The moment a pathogen crosses from an animal into a person is called zoonotic spillover, and it is the hinge on which almost every emerging infectious diseases story turns.
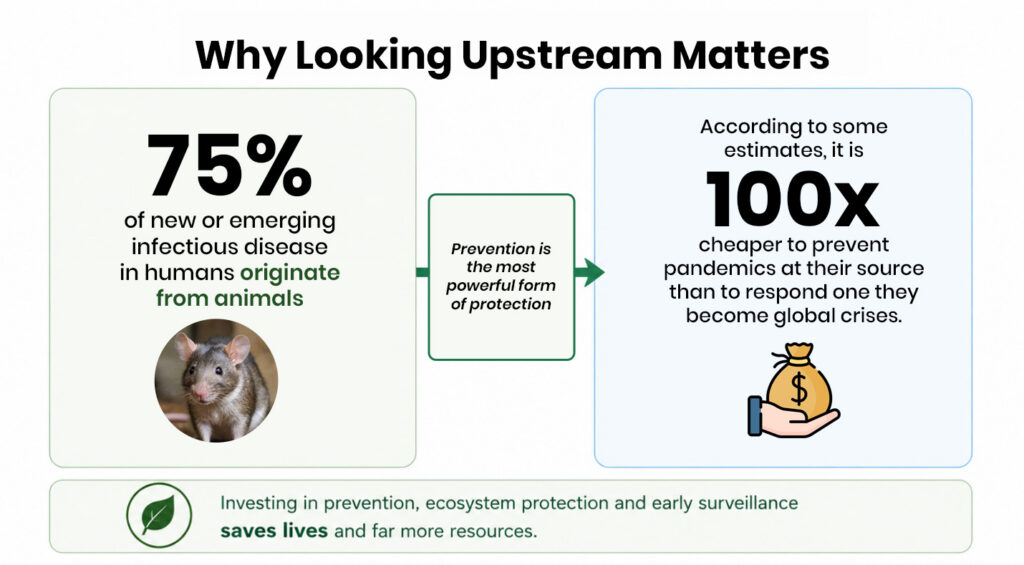
The pattern is strikingly consistent. By the reckoning of the UN Environment Programme and others, around six in ten known human infections can pass from animals, and roughly three in four new or emerging ones originate there. HIV, Ebola, influenza, SARS, MERS, Nipah, Zika – and, most scientists conclude, the virus behind COVID-19 – all trace back, directly or through an intermediary, to an animal source.
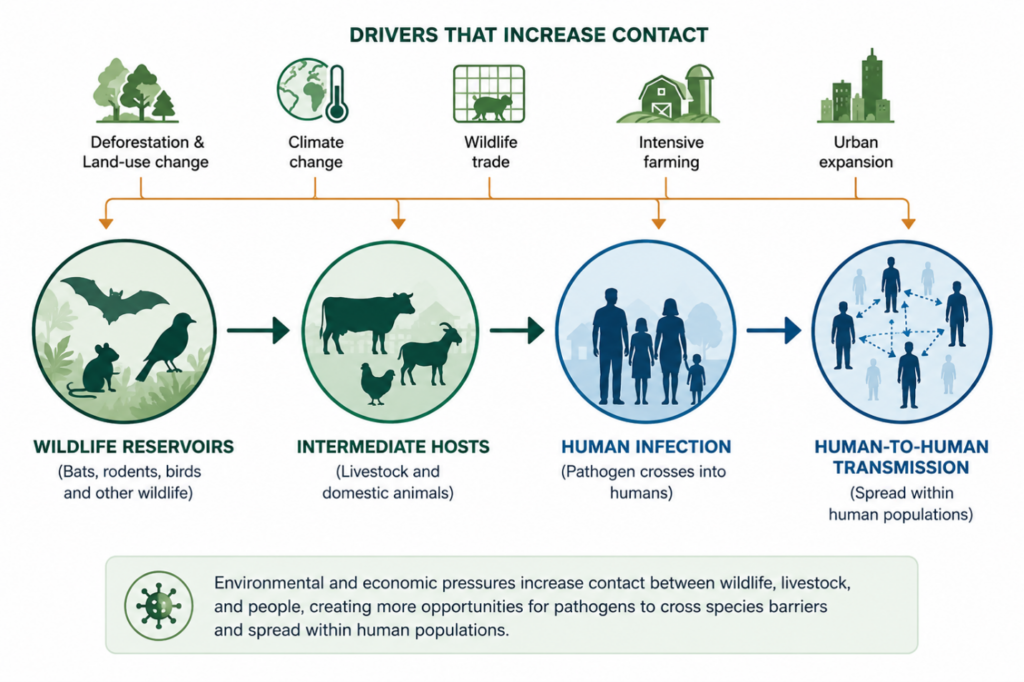
Spillover is rarely a single dramatic leap. It is more often a process of repeated contact shaped by the growing pressure of human-wildlife interaction. A virus circulates harmlessly in a wild reservoir – often bats, rodents or birds. Then it encounters people or their livestock again and again. Almost every contact goes nowhere. But each one is another roll of the dice, and the more often the dice are thrown, the greater the chance a pathogen finds the combination that lets it take hold in a human and, eventually, pass from one person to the next.
What decides how often the dice are thrown is largely us.
Consider Nipah virus. In late-1990s Malaysia, forest was cleared for industrial pig farms, and fruit trees were left standing beside the sheds. Fruit bats, pushed out of vanishing habitat, fed in those trees and dropped saliva and half-eaten fruit into the pens below. The pigs caught the virus; their handlers caught it from the pigs; more than a hundred people died. No part of that chain began in a hospital. It began at a man-made seam between forest and farm; exactly the kind of edge we are now creating, faster than ever, all over the world.
How environmental change shapes disease risk
Spillover, then, is not bad luck visited on us by nature. It is, to a significant degree, a consequence of decisions: about how we use land, raise animals, trade wildlife and heat the planet. Change the landscape, and you change the odds of emerging infectious diseases.
Deforestation is the clearest illustration. When forest is cleared for farming, mining or settlement, people and animals are pressed into the same shrinking spaces, and the buffer that once separated human and wild worlds thins to nothing. This growing human-wildlife interaction creates more opportunities for pathogens to cross species barriers. Research from the Amazon to West Africa has tied forest loss, and the ragged edges it leaves behind, to higher rates of malaria, Ebola and other diseases.
Biodiversity loss works more quietly. In many ecosystems, a rich variety of species appears to dilute disease: most species are poor hosts, and they crowd out the efficient ones. As that variety collapses, the survivors tend to be the hardy generalists; certain rodents and bats among them, that are also disproportionately good at carrying pathogens dangerous to us. Lyme disease in North America is the textbook case: fragmented woodlands, stripped of predators and diversity, tend to harbour more infected ticks.
Climate change adds a further dimension. Warming temperatures and shifting rainfall are redrawing the maps of where mosquitoes, ticks and other carriers can live, pushing diseases like dengue into new regions and higher altitudes. Climate stress also forces animals to move, bringing species together in combinations the world has never seen before.
Beneath all of it lies the sheer intensity of modern contact: industrial livestock production, wildlife markets, and a transport network that can move a virus from a rural frontier to a capital city in a single day. The World Health Organization now ranks climate change among the greatest threats to human health – and the list of forces driving spillover reads, uncomfortably, like a description of the modern economy.
If our choices raise the risk, our choices can also lower it. Spillover is not fate.
Why outbreak surveillance must move beyond hospitals
Seeing danger early is the job of surveillance, and it is here that the conventional approach meets its limits.
Classic disease surveillance begins with a sick person: they fall ill, seek care, get tested, and the result travels up a reporting chain. This machinery is indispensable and has saved millions of lives. But it shares the hospital’s blind spot. It can only detect a disease once enough people are already infected to register as a pattern – which means it always reports the past. By the time the signal is unmistakable, the pathogen has a head start measured in weeks.
It is a little like installing smoke detectors only inside the building, while ignoring the dry forest next door. By the time the alarm sounds, the fire is already in the room.
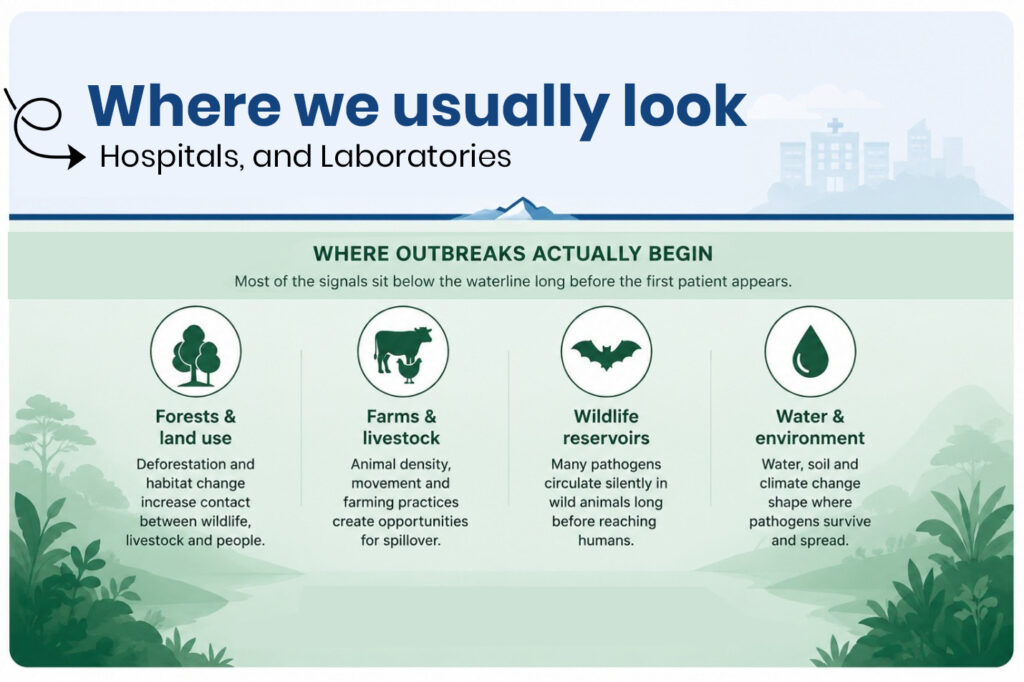
Environmental surveillance moves the detectors outside. Rather than waiting for patients, it looks for the pathogen itself: in the environment and in animals, before, or as, it reaches people. Some of the most powerful methods are also the least glamorous. Wastewater surveillance treats a city’s sewage as a single, citywide blood test: by sampling what an entire population flushes away, scientists can register a virus spreading days or weeks before individuals start seeking care. It gave many cities their earliest warning during COVID-19, and it has repeatedly caught poliovirus circulating silently in places that believed they had left it behind.
Animals are the other early page of the story. An unexplained die-off among wildlife, or a strange new infection in a herd, is often the first sentence of a threat later written in people. The recent spread of H5N1 avian influenza from wild birds and poultry into, of all places, dairy cattle, is a live reminder that the warning often arrives on four legs before it arrives on two.
None of this is meant to replace the hospital. It is meant to surround it; to turn the clinic from our first warning system into our last line of defence.
How Genomic Surveillance Is Changing Outbreak Detection
If environmental surveillance tells us where to look, genomics tells us what we are looking at, and how worried to be.
Every pathogen carries its own genetic code – a sequence that acts as both fingerprint and family tree. Genomic surveillance is the practice of reading that code at scale: identifying a microbe, mapping how it spreads, and catching the mutations that make it more dangerous. Work that not long ago demanded months and a major laboratory can now, in many places, be done in days on a sequencer the size of a stapler.
The world watched this capability prove itself in real time. In late 2021, scientists in southern Africa detected, sequenced and openly shared the genome of an alarming new coronavirus variant within days, thereby handing the rest of the planet a precious head start on Omicron. The same tools let researchers tell a routine seasonal virus from a genuine novelty, trace an outbreak back to its origin, and read, in the letters of a genome, whether a pathogen is learning to spread faster.
Crucially, these capabilities are no longer confined to a handful of wealthy countries. Sequencing networks have expanded across Africa, Asia and Latin America, and initiatives now link laboratories so that a signal detected in one country can inform the response everywhere. Biotechnology has, in effect, given public health a faster pair of eyes. Increasingly, these tools are being used far beyond traditional clinical settings. Researchers are applying genomic technologies to wastewater, wildlife populations, and environmental samples to identify pathogens before they become widespread human health threats.
This marks an important shift in public health thinking: from responding to outbreaks after they occur to identifying risks earlier and intervening before they escalate. In many ways, genomics is helping move disease surveillance upstream, closer to where outbreaks actually begin. The challenge is making sure those eyes are pointed at the right places, and that every region can afford to keep them open.
The One Health Approach to Pandemic Prevention
Follow these threads far enough and they converge on a single, almost disarmingly simple idea: human health, animal health and environmental health are not three problems but one, seen from three angles. This is the principle known as One Health
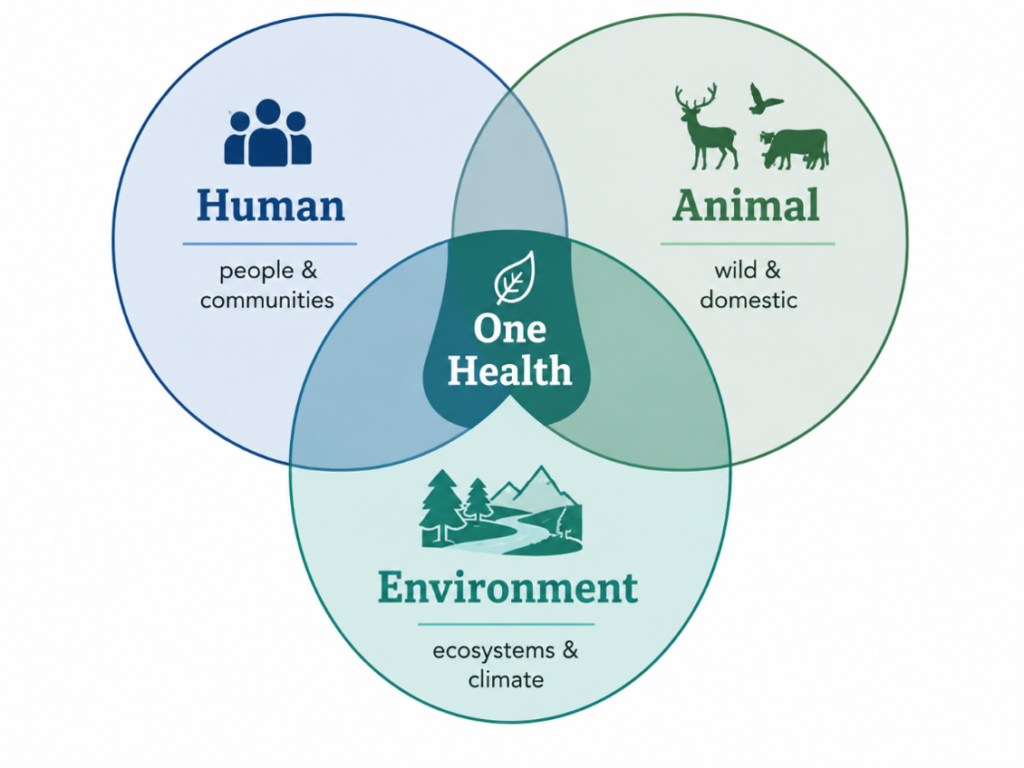
One problem, three angles. Healthy people depend on healthy animals and healthy ecosystems. The One Health approach recognises that protecting one means protecting all..
One Health holds that we cannot keep people well while the animals and ecosystems we depend on are sick. In its light, a vet puzzling over dying livestock, an ecologist tracking a stressed bat colony, a clinician facing an unfamiliar fever and a technician reading a city’s wastewater are all doing the same work: public health, even though they have traditionally sat in different ministries, drawn on different budgets and spoken different professional languages. The quiet revolution of One Health is, in large part, simply about making those people talk to one another.
The world’s major health and environment bodies are, belatedly, catching up. The WHO, the Food and Agriculture Organization, the World Organisation for Animal Health and the UN Environment Programme now operate as a “Quadripartite,” steered by a joint expert panel on a shared One Health agenda.
Initiatives such as PREZODE (Preventing Zoonotic Disease Emergence ) link scientists and frontline communities across dozens of countries to stop spillover at its source. And in May 2025, after more than three years of negotiation, the World Health Assembly adopted the world’s first Pandemic Agreement, placing strengthened surveillance and a One Health approach at the centre of how nations intend to keep the next outbreak from becoming the next pandemic.
The logic is not only ethical but economic. Analysts have repeatedly found that preventing pandemics at their source costs a fraction – by some estimates around a hundredth – of what it costs to respond once an outbreak has gone global.
Prevention is not the expensive option. Measured against the alternative, it is the bargain of the century.
Why This Matters Now
The need to rethink where future disease threats begin has never been more urgent. Around the world, climate change is altering ecosystems, changing wildlife migration patterns, and influencing the distribution of disease vectors such as mosquitoes and ticks. At the same time, expanding agriculture, urbanisation, and land-use change are increasing contact between humans, livestock, and wildlife, creating new opportunities for pathogens to cross species barriers.
Recognising these risks, governments, international organisations, and research institutions are investing more heavily in the One Health approach, which promotes collaboration across human, animal, and environmental health sectors. Recent global initiatives, including the WHO Pandemic Agreement, reflect a growing consensus that preventing future outbreaks requires stronger surveillance systems, greater international cooperation, and earlier detection of emerging threats.
Advances in genomic sequencing, environmental monitoring, artificial intelligence, and real-time disease surveillance are also transforming our ability to identify risks before they become crises. Together, these developments signal an important shift in global health: from reacting to outbreaks after they occur to understanding and addressing the conditions that allow them to emerge in the first place.
| A QUICK GLOSSARY Four ideas, in plain language Zoonotic spillover The moment a disease passes from an animal into a human. It is the starting gun for most new outbreaks. Environmental surveillance Watching for pathogens in the environment and in animals. For example, in wastewater or wildlife, rather than waiting for sick patients. Genomic surveillance Reading a pathogen’s genetic code to identify it, track its spread, and detect dangerous changes early. One Health The approach that treats human, animal and environmental health as a single, connected system |
What this means for communities
It would be easy to read all this as the work of distant institutions. It is not. Communities are often portrayed as passive recipients of public health interventions, yet they are frequently the first to notice when something unusual is happening. Farmers may observe changes in livestock health, rangers may witness unexpected wildlife deaths, and community health workers may encounter unfamiliar symptoms before they appear in official surveillance data. These observations, when supported by strong reporting systems and trusted institutions, can provide invaluable early warnings.
This highlights an often-overlooked reality: effective disease prevention depends not only on technology and laboratories, but also on local knowledge, community engagement, and public trust. The sooner unusual events can be recognised and communicated, the greater the opportunity to prevent local incidents from becoming larger public health emergencies.

For policymakers, the lesson is to stop filing health, agriculture and the environment in separate drawers. Protecting a forest, regulating a wildlife market, supporting sustainable farming and funding a diagnostic laboratory are all, properly understood, pandemic-prevention measures. For NGOs and public health bodies, the work is to build the bridges: between sectors, between disciplines, and between the global laboratory and the local knowledge that will always notice something first.
And for the rest of us, it asks only a small shift of imagination: to see that the health of a far-off rainforest or a distant herd is quietly, stubbornly bound up with our own.
So, are we looking in the right places?
For much of the last century, the honest answer has been: not quite. We built a remarkable system to detect and treat disease once it reaches us, and a far weaker one to see it coming. We have been watching the hospital door while the real action unfolds upstream, in the forests we clear, the climates we unsettle and the animals we crowd against.
What has changed is that looking upstream is no longer a wish; it is a choice we are now equipped to make. Sewage can warn us before patients do. A genome can be read and shared around the world in a day. One Health is dismantling the walls between human, animal and environmental medicine, and for the first time the world has a treaty that takes prevention as seriously as cure. The instruments are in our hands; what remains uncertain is where we decide to point them.
Because the next outbreak is not a matter of if but of when. Whether it stays a local tragedy or becomes a global one may hinge on a decision we are making right now, mostly without noticing it – to keep waiting at the clinic door, or to turn around and watch the places where the next outbreak is, even as you read this, quietly taking shape.
Preparing for future outbreaks will require more than stronger hospitals and faster diagnostics. It will require a broader understanding of health itself; one that recognises the connections between people, animals, and the environments they share. The most effective public health systems of the future may not be those that respond fastest to disease, but those that are able to recognise risk early enough to prevent outbreaks from occurring in the first place
The right places are not a mystery. The only open question is whether we will choose to look. ◆
About this article.
This article was written by Oluchi Adaku Agbo for the Batnon Centre for Environment and Sustainable Development. Drawing on perspectives from public health, biotechnology, and environmental health, it explores how emerging disease threats are increasingly shaped by the interactions between people, animals, and ecosystems. The article forms part of Batnon’s ongoing effort to promote accessible, evidence-based discussions on public health, sustainability, and community wellbeing. Figures are illustrative. Key reference points include the WHO Pandemic Agreement, the Quadripartite One Health framework (WHO, FAO, WOAH, UNEP), and the international PREZODE initiative.